

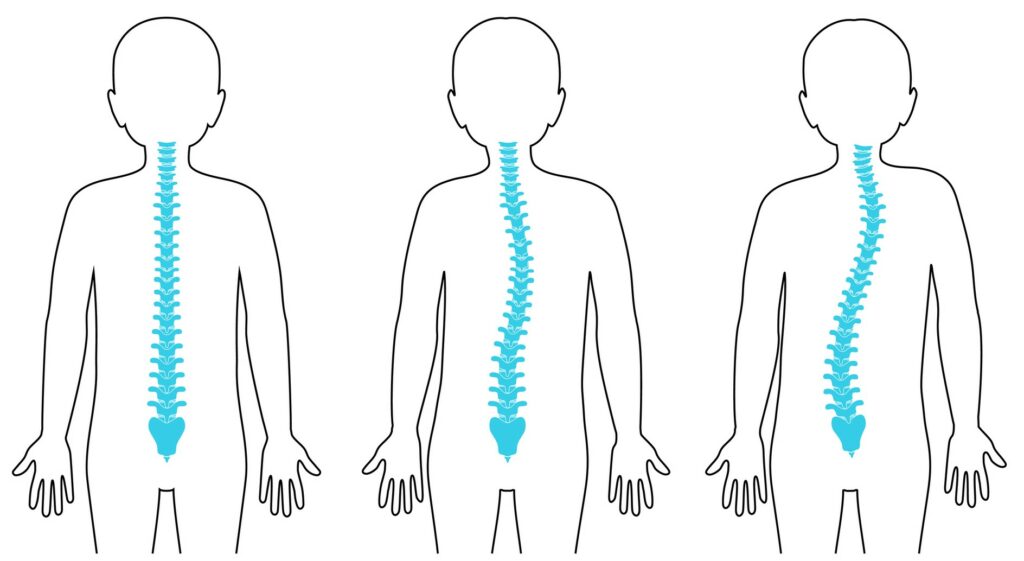
Scoliosis, an abnormal curvature of the spine, affects two to three percent of the population, representing an estimated six to nine million people in the U.S., according to the National Scoliosis Foundation. Most affected are:
- Girls, who are seven times more likely to develop scoliosis than boys.
- Heredity plays a role –a mother or father who has a parent or first-degree relative with scoliosis has a 50 percent chance of having a child with scoliosis.
- Maternal age is a factor – A mother who gives birth after the age of 27 has a greater risk of having a child that develops scoliosis as a result of a spontaneous mutation, as reported in the Journal of Bone and Joint Surgery.
Curvature of the spine can affect anyone. Athletes like Olympic swimmers Jessica Ashwood and Aritza Correia, and professional golfer Katie Webb, actresses Daryl Hannah, Elizabeth Taylor and Liza Minelli, and well-known figures like General MacArthur and Egyptian Pharoah Tutankhamun all had scoliosis.
Detecting Scoliosis in Children
Scoliosis can develop in infancy, early childhood, and adolescence but the older the child, the more difficult it can be to diagnose. It is easier to diagnose the condition in younger children because a parent bathing a child between infancy and age three may notice an emerging problem, or a pediatrician will identify juvenile scoliosis in children age three to 10. But in children 11 years old and up, it can be more difficult to diagnose because they are more self-conscious about body image, which is precisely why your child’s school screening program or annual pediatric physical are keys to early detection—which can lead to early intervention.
Scoliosis is not always idiopathic. Some of the warning signs that scoliosis is caused by a more serious issue is if the child has scoliosis and a hairy patch or dark brown lesions on your child’s back; back pain which is localized or wakes the child from sleep, urinary incontinence or retention, constipation or bowel incontinence. These are all signs that further evaluation by an orthopedist who specializes in diagnosing and treating scoliosis is in order.
The sooner a child is formally diagnosed and begins treatment for scoliosis, the more likely the treatment will be less aggressive and the child can avoid surgery.
“I have always said that I treat my patients as I would my own child, a fact that perhaps resonates even more because my daughter has scoliosis and was treated successfully with bracing as a child,” stated Dr. Rieger. He continues, “This is why I am especially averse to subjecting children to unnecessary amounts of radiation from X-rays and why I highly recommend parents seek out physicians with access to low-dose radiation technology such as the EOS Machine as part of the diagnostic process.”
Scoliosis Treatment Options for Children
Once an orthopedist has confirmed the diagnosis of scoliosis, they will determine if treatment is required and what kind of treatment is best suited to your child’s condition.
Non-surgical treatments
- If the spinal curves are small, we may recommend dietary supplements with vitamin D and calcium.
- Larger curves in the spine are treated using another non-invasive treatment called Schroth therapy, an exercise program that teaches children how to breathe, stretch and strengthen their spine to counter the impact of their scoliosis. These two treatments are designed to prevent scoliosis’ progression.
- If a child’s spinal curve progresses, the pediatric orthopedist will likely add nighttime or full-time bracing. The question “For how long?” always arises. Girls will typically wear the brace for two years from the onset of menses; boys, for two years from the time they have a major growth spurt. But the earlier the diagnosis, the less likely your child will require bracing or they may be able to wear the brace only at night.
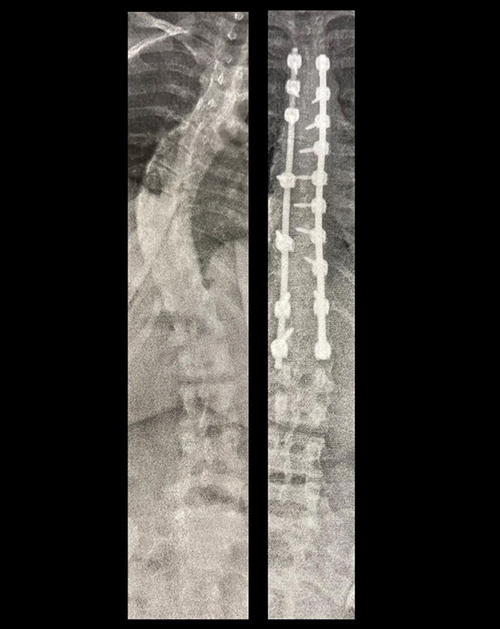
Scoliosis Surgery
- While 95% of children can avoid surgery by initiating early treatment, spinal fusion surgery is reserved for the most severe cases of scoliosis in adolescents. Surgical advances mean that typical hospitals stays are only two days, with children able to return to some activities in approximately six weeks and almost all their activities by three months.
- A new scoliosis surgical advancement called anterior vertebral tethering allows pediatric orthopedic surgeons to modulate the growth of the spine so it corrects gradually over time and preserves spinal motion. It, unfortunately, has a 20% reoperation rate compared to fusion, which has a less than 1% reoperation rate
The diagnosis and treatment of scoliosis has evolved and helps children resume their normal activities and live a better quality of life. Talk to your child’s physician about evaluating them for scoliosis at their next wellness visit.
To reach The Pediatric Orthopedic Center, please click here or call (973) 538 – 7700
For further information, please view our video featuring our very own Dr. Mark Rieger!


